Future of Healthcare’s Clinical Workforce
Wave Labs convened payers, providers, entrepreneurs, and policy leaders on May 14 to tackle one of healthcare's most consequential questions. Here's what we learned.
The doctor will see you now. Except the doctor might be a large language model, a computer vision system trained on 100 million retinal scans, or a deterministic clinical engine enrolled in nursing school. That is not hyperbole — those are actual companies that presented at our May 14 Wave Labs event on the Future of Healthcare's Clinical Workforce. And the conversation they sparked was one of the most substantive we have had yet.
Wave Labs brought together a room of payers, providers, technologists, entrepreneurs, academics, and policy leaders to pressure-test where AI fits in clinical care delivery — not the usual hand-wavy optimism about transformation, but the real questions: Who's liable when an AI prescribes the wrong drug? Can a regulator license software the same way it licenses a physician? And why do the companies saying "we replace clinicians" keep outperforming the ones saying "we augment them" — at least in some markets?
The Setup: A Shortage That's Not Waiting for Clarity
SpringTide's Gabi Tallez opened with the market context. Healthcare is staring down a widening clinical workforce shortage — a gap that was already structural before COVID accelerated burnout and early retirement. Meanwhile, the technology catching up to the problem is moving faster than most institutions realize.
Conversational AI has crossed a threshold. Agentic systems can now conduct intake interviews, synthesize patient histories, flag drug interactions, and generate clinical documentation at a level that is no longer just "good enough to test." It is good enough to deploy. Add to that a generation of younger patients who already manage their health through smartphones — who Googled their symptoms before calling a nurse, who prefer async messaging to a 15-minute appointment — and the adoption curve looks less like a question of whether and more like a question of who governs it.
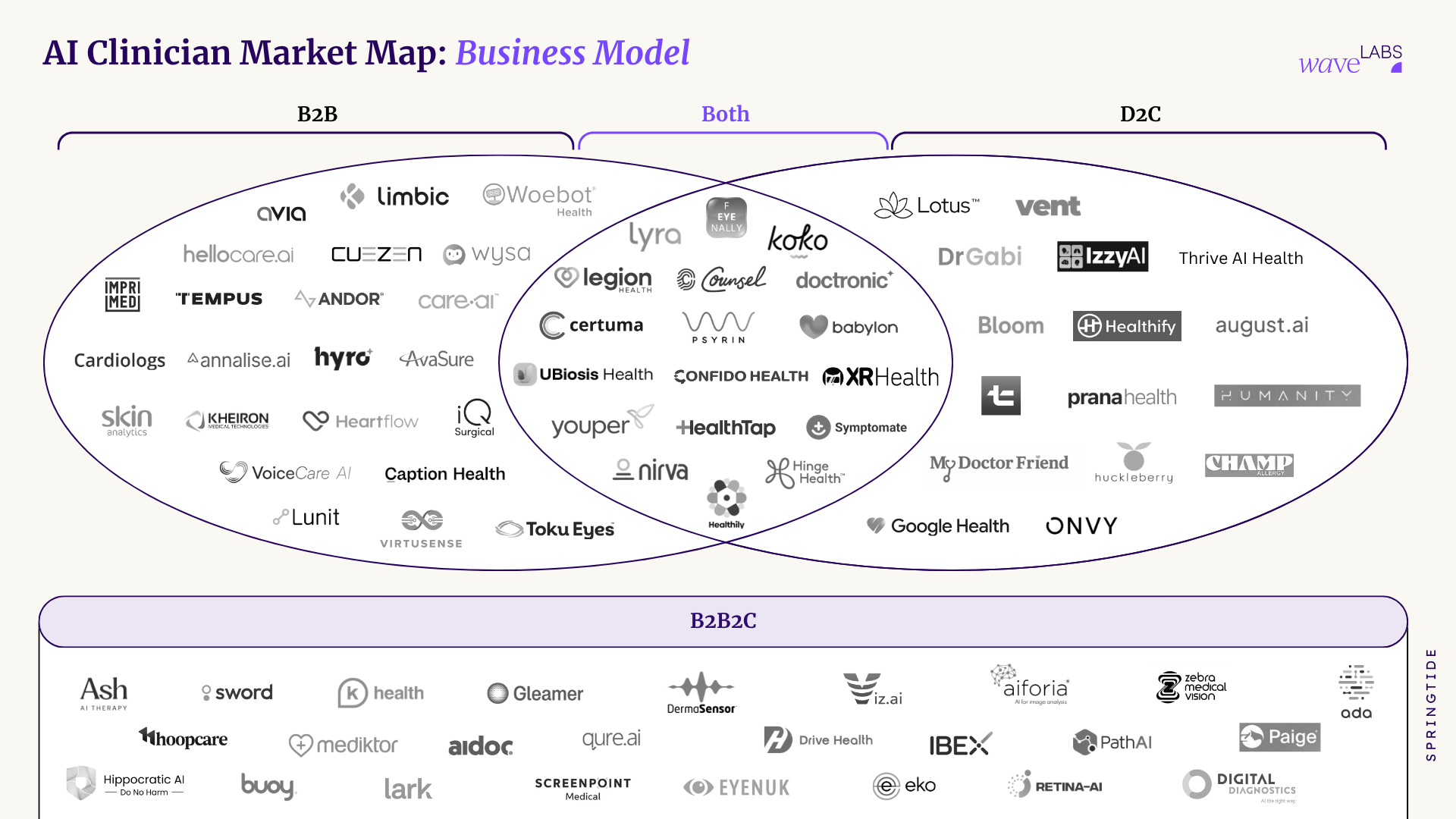
The Business Model Tension
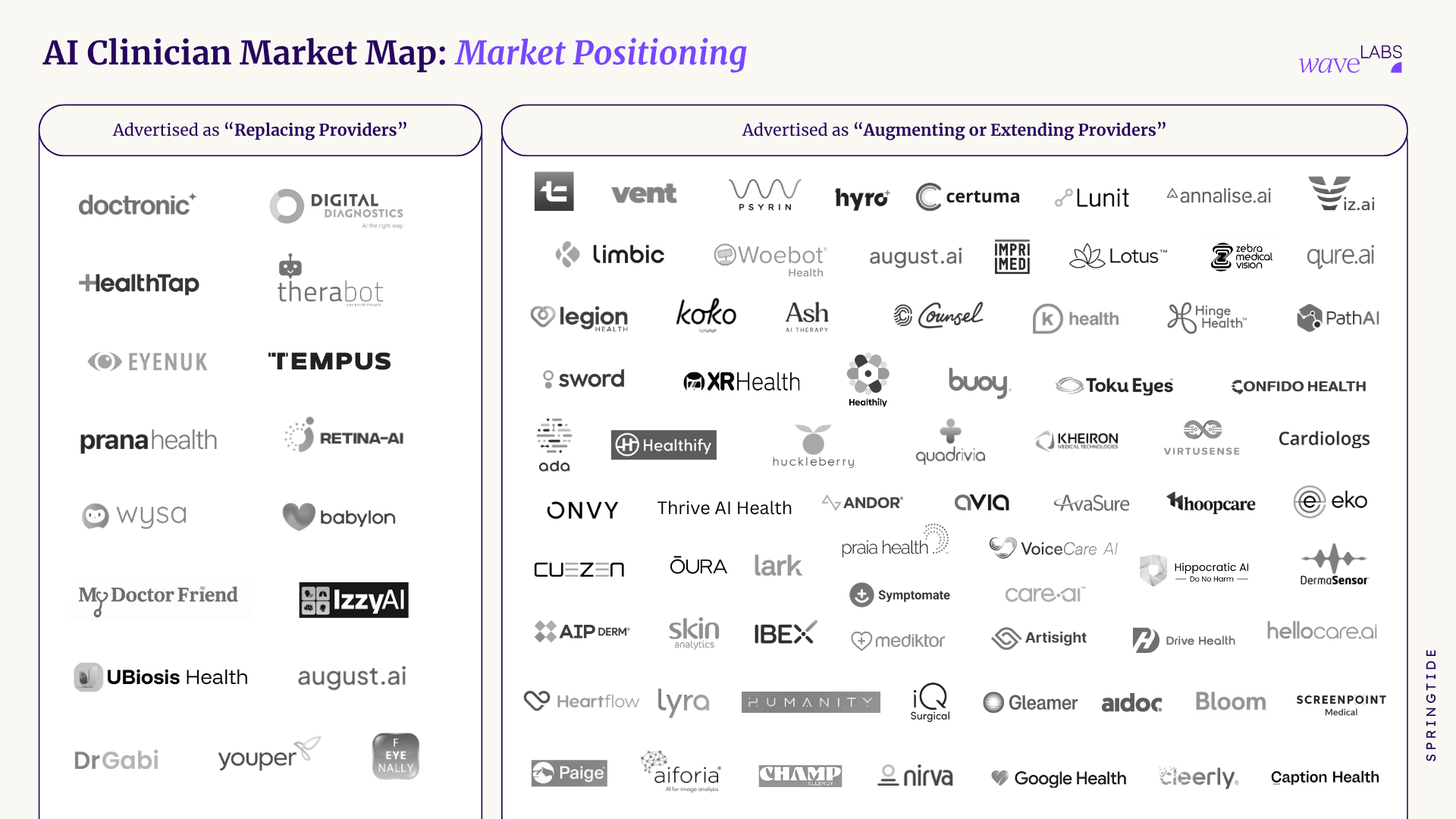
One of the sharper threads of the session: the language companies use to describe their products is not just marketing — it is a strategic lever that shapes procurement, regulation, and growth trajectory in fundamental ways.
B2B buyers — health systems, insurers, large employers — strongly prefer the word augment. When a vendor says their AI augments clinical workflows, procurement moves faster, ROI is easier to model, and the regulatory burden stays manageable. Hospital administrators are not eager to sign contracts that could expose them to liability for a system described as replacing clinical judgment.
Direct-to-consumer is the mirror image. D2C companies positioning their products as replacing the need for a traditional clinical encounter — skipping the waiting room, skipping the referral, getting a prescription renewed at 11 PM — are finding strong consumer resonance. Patients, especially underserved ones with limited access to care, are not particularly attached to the incumbent model.
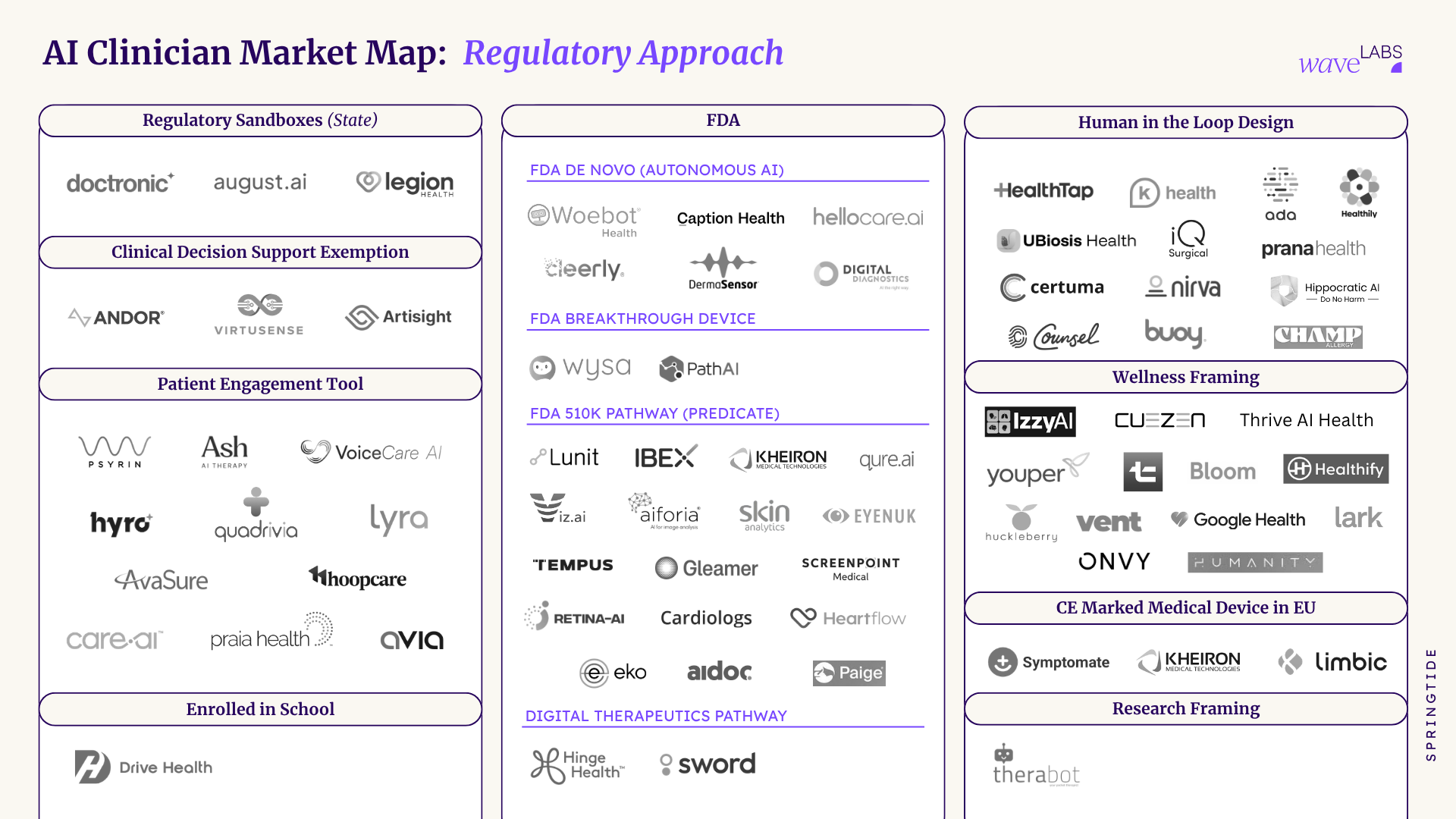
The takeaway is not that one positioning is right. It is that the same underlying technology can be packaged either way, and the choice has downstream consequences for everything from fundraising to FDA classification to which customer segment you can realistically close. Companies that haven't thought carefully about this are making the decision by default.
The second business model insight was equally pointed: technology alone does not build a moat. The AI scribing market is the cautionary tale. Ambient documentation was a genuinely hard technical problem until it was not — now it is approaching commodity status, with dozens of vendors competing on price. The same pattern is likely to play out in triage, patient engagement, and diagnostic support. The companies that will build durable businesses are not just the ones with the best models. They are the ones pairing the model with distribution advantages, sticky workflows, proprietary data, or regulatory positioning that competitors cannot easily replicate.
The Regulatory Puzzle: Can You License an Algorithm Like a Doctor?
This was the deepest conversation of the afternoon, and it surfaced two genuinely distinct frameworks worth understanding.
Eric Brussman (UPenn) made the case for treating AI clinical systems the way we treat human clinicians: licensing them. His framework would require AI systems to meet pre-entry practice standards before deployment, move through a supervised apprenticeship period operating under human oversight, and remain subject to ongoing monitoring with real disciplinary authority — the ability to revoke or restrict a system that causes harm. The intuition is that if an AI is making the kinds of decisions a physician makes, it should face the same accountability structure. The current FDA software-as-medical-device framework, designed for static software, is structurally inadequate for generative AI that updates, evolves, and behaves differently across patient populations.
Zach Boyd (Utah AI Policy) came at it from a governance angle. Rather than mapping to professional licensing, his approach emphasizes pre-deployment safety review, evidence generated through real-world deployment under controlled conditions, and elevated post-market surveillance — particularly important for AI systems that are not static products. They change. They can drift. Monitoring after launch is not a bureaucratic formality; it is the primary safety mechanism.
Both frameworks share an underlying premise: the current regulatory toolbox does not fit. What they disagree on is whether the solution is to build a new track that mirrors clinical credentialing, or to build a governance infrastructure that treats AI as a different kind of entity requiring a different kind of oversight.
The Utah Sandbox: The Pilot Everyone Is Watching
The most concrete regulatory development discussed was the Utah AI sandbox pilot involving Doctronic, which has been approved for a narrow but significant use case: prescription renewals. Not new prescriptions — renewals. And not without oversight: Phase 1 requires one to two humans reviewing every AI-generated decision before a prescription is generated.
That sounds modest. The significance is in what it represents. Utah is the first U.S. state to formally create a pathway for AI to participate in a prescribing workflow, even a tightly bounded one. The pilot sparked immediate public debate — strong reactions in both directions — which is itself a signal that the question of AI in clinical decision-making has crossed from industry conversation into public consciousness.
What happens in Utah matters beyond Utah. A clean pilot with good outcomes creates a template other states can follow and gives companies in this space a regulatory proof point. A high-profile failure — a prescription error, a safety incident, a patient harmed — could set back the entire category. The stakes for early regulatory pilots are not symmetric.
Five Companies Building the Future (Right Now)
The company showcase portion of the session put concrete shape on what is actually shipping, not just what is being theorized.
Doctronic (Greg Fitzgerald) is positioning as AI-native primary care: 24/7 physician access with a 30-minute SLA for response. The pitch is that primary care does not need to be scarce if the system is redesigned around AI-assisted triage and clinical support.
Feyenally (Nastazja Puzinowska) is building an AI optometrist using smartphone photos to conduct eye exams — targeting a $15B global market where access to optometrists is severely constrained, particularly in lower-income and rural populations. The smartphone is the distribution layer that makes this possible at scale.
IQ Surgical (Jay Park) is focused on neurosurgery — specifically, building a real-time AI copilot for surgical procedures and constructing what they describe as a surgical intelligence data layer. The wedge is making surgeons safer and faster; the long-term asset is the proprietary data.
Drive Health (Kevin Longoria) introduced Nurse Avery, an AI nurse enrolled at Arizona State University's nursing school. The technical differentiator is a deterministic clinical engine claiming a 0% hallucination rate — a significant claim in a domain where hallucination is a genuine patient safety risk, not just an inconvenience.
August AI (Anuruddh Mishra) has scaled to 8 million users across 160 countries and is running what they describe as a continuous virtual residency — essentially ongoing real-world testing of the AI system's clinical reasoning across a global patient population.
The Durable Insight
Across the business models, the regulatory frameworks, and the company showcases, one theme held: the companies and institutions that will shape this space are not the ones building the most capable AI. They are the ones building around the AI — solving the distribution problem, constructing the regulatory strategy, earning the patient trust, and creating the data infrastructure that makes a model more accurate over time.
Agentic solutions are not a business. They are a component. What you build around them is the business.
What's Next
This session was the first in a series. Upcoming Wave Labs events will tackle the human clinician perspective — what physicians, APPs, and nurses actually think about working alongside AI systems — and the pace of underlying technology advancement and what it means for the architecture of care.
If these conversations are the ones your organization needs to be part of, watch the full recording here and download the event one-pager here.
Wave Labs is SpringTide's ongoing series convening leaders at the intersection of technology, care delivery, and healthcare policy. Join the Wave Network to be part of future sessions.